Back Pain Why it Hurts

Anatomy & the surprising mechanics of back pain (back pain, low back pain)
Your spine: small parts, big signals
Your spine is a stack of bones with discs (shock absorbers) between them, facet joints (small guiding joints) at the back, and a web of muscles and nerves around it. When any of these tissues are irritated, your nervous system can turn up the alarm. That is why back pain can feel intense even when scans show only minor changes.
Low back pain is often labelled non-specific low back pain, meaning there is no single clear structural cause. In many people, pain relates more to how the back is being loaded and protected than to one “damaged” part.
Motor control: why movement patterns matter
Motor control is how your brain and muscles coordinate to keep you steady during daily tasks. If timing is off—say, your deep trunk muscles switch on late—other tissues may take extra strain. Over time, this can keep pain active even without ongoing injury.
Research also suggests that non-specific low back pain can cluster with features like motor control issues and even neck pain, which supports the idea that the whole movement system matters.
Neuropathic pain: when nerves join in
Sometimes pain is partly neuropathic pain, where irritated nerves create burning, tingling, or shooting symptoms. This does not always mean serious damage, but it can change how you move and guard your back.
Why “sit less” can feel too simple
Posture is only one piece of the puzzle. Sitting can be uncomfortable, but so can standing still. Often, the issue is staying in one position and how well you share load through hips, trunk, and legs.
2) Common causes, myths and the role of chronic pain (chronic pain, pain management)
Acute mechanical back pain vs chronic pain
Your back can hurt for simple, short-term reasons. Acute mechanical causes include a muscle sprain, a joint irritation, or a disc “flare” after lifting, twisting, or a sudden increase in activity. These episodes often settle as tissues calm down and you rebuild movement confidence.
Chronic pain is different. When pain lasts beyond normal healing time, your nervous system can become more protective and sensitive. This helps explain why research keeps placing pain, chronic pain, and low back pain among the most studied terms (2017–2021 strength metrics: pain 66,282; chronic pain 22,376), and why newer hotspots focus on non-specific low back pain and management strategies (keyword bursts 2014–2023).
Myth: “My scan shows degeneration, so my back is damaged”
Scans often show age-related changes (like “degeneration”) even in people without symptoms. Imaging can be useful, but it is not the whole story. Pain levels do not always match what a scan reports, especially in chronic pain where sensitisation matters.
A gardener once told me his scan said “degeneration”, and he feared he was “wearing out”. With targeted exercise and clear education, he halved his pain score.
When neuropathic pain is part of the picture
Sometimes nerve-related symptoms dominate. Neuropathic pain may feel like burning, electric shocks, pins and needles, or numbness, often with pain travelling down the leg. This can change your pain management plan and may warrant earlier clinical review.
Practical pain management principles (including opioid use context)
-
Keep moving: use gradual activity rather than rest.
-
Graded exercise: build tolerance in small, planned steps.
-
Calm the system: sleep, stress reduction, and pacing support recovery.
-
Osteopathy and Acupucture: consider simple options first; be cautious with opioid use in chronic pain due to limited long-term benefit and higher risk.
-
Refer when needed: worsening weakness, bladder/bowel changes, or persistent neuropathic pain symptoms should prompt MRI and referral.
3) Simple steps you can try and when to get help (pain relief, low back pain management)
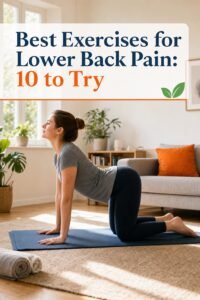
Start with targeted movement for pain relief
If your back hurts, begin with gentle, targeted exercise rather than rest. Many people have small motor control deficits, where the muscles that support your spine do not switch on well. Simple muscle strengthening and core stability exercises can improve control and reduce flare-ups. Start with short sessions, keep the movement smooth, and increase only when symptoms settle within 24 hours.
Self-management that supports low back pain management
For day-to-day low back pain management, use pacing: break tasks into smaller blocks, change position often, and plan recovery time. Protect your sleep with a steady bedtime, a cool dark room, and less screen time late on. Stress can raise pain sensitivity, so add a brief daily routine such as slow breathing or a short walk. If you use an app, choose vetted mHealth apps that offer graded exercise plans and clear safety advice; track your hours/week of use and note any symptom changes so you can see what helps.
When to get help
Try non-invasive options first: graded exercise, education, heat, Osteopathy or Acupuncture. Seek urgent assessment if you develop progressive weakness, bowel or bladder changes, or severe unrelenting pain. Getting the right support early helps you stay active, choose evidence-based care, and avoid unnecessary invasive treatments.