You wake up stiff. The first few steps to the kitchen feel awkward. Stairs make you hesitate. Getting out of the car takes planning. By the end of the day, your joint feels used up, but sitting still for too long makes it worse again.
That’s where many people start when they search for osteoarthritis treatment uk. They’re not looking for theory. They want to know what helps, what’s available on the NHS, what has to be done privately, and what to do when simple advice hasn’t solved the problem but surgery feels far too big a step.
You’re far from alone. Approximately 1 in 5 adults over 45 in England have knee osteoarthritis (18.2%), and 1 in 9 have hip osteoarthritis (10.9%), according to Arthritis UK local authority estimates for England. That matters because it shifts the problem from “just me getting older” to a common, treatable condition that deserves a proper plan.
Clarity matters. Osteoarthritis care in the UK is broad, but confusion typically arises in the middle ground: after self-care has started, before major interventions make sense.
Table of Contents
- Living with Joint Pain and Seeking Clarity
- What Is Osteoarthritis and How Is It Diagnosed
- Your First Steps for Managing Osteoarthritis Pain
- Evidence-Based Non-Surgical Treatments
- Navigating NHS vs Private Osteoarthritis Care
- When to Consider Injections and Joint Surgery
- Your Osteoarthritis Questions Answered
Living with Joint Pain and Seeking Clarity
A common pattern goes like this. Someone notices a sore knee after walks, then avoids hills, then starts using the banister on stairs, then realises they’re planning their day around pain. Another person finds their hip is worst first thing in the morning, loosens after moving, then aches again after sitting at a desk or driving.

That’s often how osteoarthritis behaves in real life. It rarely feels dramatic at the start. It feels persistent, limiting, and irritatingly inconsistent. Good days make you think it’s easing. A bad week makes you worry it’s getting out of control.
The practical problem most people face
What unsettles people isn’t only pain. It’s uncertainty. They’re told to keep active, but movement hurts. They hear about scans, injections, surgery, supplements, braces, insoles, physiotherapy, acupuncture, and hands-on treatment, yet nobody seems to explain how these fit together.
You don’t need a perfect diagnosis story or a severe X-ray to justify getting help. You need a clear assessment and a sensible next step.
The useful question isn’t “What is the one treatment?” It’s “What is the right treatment at my stage, for this joint, with this level of pain and function?”
What a good plan should give you
A good osteoarthritis plan should help you answer three things:
- What’s likely driving the pain: joint irritation, stiffness, weakness, overload, or a mix of these.
- What you can do yourself: movement, pacing, strength work, and symptom control.
- When to escalate: to practitioner-led care, injections, or an orthopaedic opinion.
Individuals typically do not need to jump straight to surgery. Many also need more than “just live with it”.
What Is Osteoarthritis and How Is It Diagnosed
Osteoarthritis is often described as “wear and tear”, but that phrase is too blunt to be useful. A better way to think of it is a joint’s wear and repair system becoming unbalanced over time. The cartilage, bone, joint lining, muscles, and surrounding tissues all respond to load. When that system stops coping well, pain, stiffness, swelling, and reduced confidence in movement can follow.
A joint under strain
Osteoarthritis doesn’t only mean cartilage loss. In clinic, the person’s experience usually comes from a combination of reduced joint tolerance, muscle weakness, altered movement patterns, and sensitivity after repeated irritation. That’s why two people with similar scan findings can feel very different.
Common signs include:
- Pain with loading: walking, stairs, standing from a chair, kneeling, or gripping.
- Short-lived stiffness: often worse after rest or in the morning.
- Reduced movement: the joint doesn’t bend, straighten, or rotate as freely.
- A gradual loss of trust: you stop using the joint naturally.
That differs from inflammatory arthritis, where symptoms may include more obvious heat, prolonged morning stiffness, multiple swollen joints, or systemic illness. If symptoms don’t fit the usual osteoarthritis pattern, further medical assessment matters.
How diagnosis usually happens in the UK
In the UK, diagnosis is often clinical. A GP, physiotherapist, or osteopath will usually listen to the pattern of symptoms, ask what aggravates or eases them, and examine how the joint moves, how you walk, and how the surrounding muscles function.
Scans can help, but they aren’t always the first step. Many people assume they need an X-ray or MRI immediately. Often they don’t. A good clinician can identify probable osteoarthritis from history and examination, then decide whether imaging would change management. If you’re unsure how those tests differ, this guide on MRI and X-ray differences in musculoskeletal assessment gives a practical overview.
Clinical reality: a scan can confirm changes in a joint, but it won’t tell you on its own which movements are poorly tolerated, which muscles need work, or why stairs are harder than flat walking.
A useful assessment should end with something concrete: what the working diagnosis is, what else needs ruling out, and what you should do next week, not just next year.
Your First Steps for Managing Osteoarthritis Pain
You wake up, the joint feels manageable, and by late afternoon it is stiff, sore, and unreliable again. That pattern is where many people get stuck. They are not ready for surgery, but simple advice like “keep active” is too vague to help. The first step is to make the joint more tolerant of daily life, not to chase a pain-free week straight away.
Effective osteoarthritis care starts with simple, consistent actions. The trade-off is that they are rarely dramatic, and they work best when adjusted to what your joint can currently tolerate.
Start by adjusting load, not stopping life
The joint usually needs better dosing, not complete rest. Full rest often increases stiffness, reduces muscle support, and makes normal movement feel less safe when you start again.
A practical starting point is to change one part of the activity that flares you. Reduce distance, slow the pace, break tasks into shorter bouts, or choose flatter ground for a couple of weeks. That keeps you active without repeatedly provoking the same flare pattern.
Build support around the joint
Stronger muscles help absorb load that would otherwise irritate the joint. What matters depends on the area involved.
- For knee osteoarthritis: quadriceps, glutes, and calves usually need attention.
- For hip osteoarthritis: glutes and hip stabilisers often make the biggest difference to walking and stairs.
- For hand osteoarthritis: grip strength, finger movement, and pacing repetitive tasks are often more useful than forcing stretches.
This is also why generic exercise sheets sometimes fall flat. The right exercise is the one you can repeat consistently, with symptoms that settle rather than spiral.
Keep some aerobic movement in the week
Walking, cycling, swimming, and cross-training can all work. The best option is the one your joint tolerates well enough to do again in two days, not the one that looks ideal on paper.
Short, regular sessions often beat occasional hard efforts.
If body weight or diet is part of the picture, address it without turning it into a blame issue. Less load through a painful joint can help, and some people notice that food choices affect how they feel day to day. If you want practical guidance, this guide to foods that may support osteoarthritis management is a sensible starting point.
Use pain relief to support function
Pain relief has a place, especially if it helps you sleep, walk, or keep up with exercise. It works best as support for a broader plan rather than the whole plan.
Practical options include:
- Topical pain relief: often a sensible first option when you want local symptom relief with less whole-body exposure than tablets.
- Oral pain relief: can help you stay active, but it needs proper medical guidance, especially if you have stomach, kidney, heart, or blood pressure issues.
- Heat or cold: simple measures that can reduce stiffness or calm a flare, depending on what you respond to.
In a European cohort including UK patients, opioids were prescribed to 51% of individuals with osteoarthritis, often after several other medications had already been tried, as reported in this European and UK prescribing analysis. In practice, that is a warning sign. If treatment keeps returning to stronger painkillers without improving function, the wider plan needs reviewing.
A simple rule for judging activity
Use your symptom response over the next 24 hours.
- If pain settles back to baseline by the next day: the dose was probably reasonable.
- If pain stays raised for several days: the activity was too much for now.
- If you are starting to avoid ordinary movement: get a more structured plan from a clinician.
Practical rule: choose activity that challenges the joint enough to maintain strength and confidence, but not so much that it triggers a prolonged flare.
That middle ground is where early progress usually happens.
Evidence-Based Non-Surgical Treatments
A common pattern looks like this. You have already tried pacing activity, simple pain relief, and the advice you were first given, but the knee still swells after a walk, the hip stiffens after sitting, or the hand pain wakes you at night. You are not ready for surgery, and you do not want to drift into months of stronger painkillers without a plan.
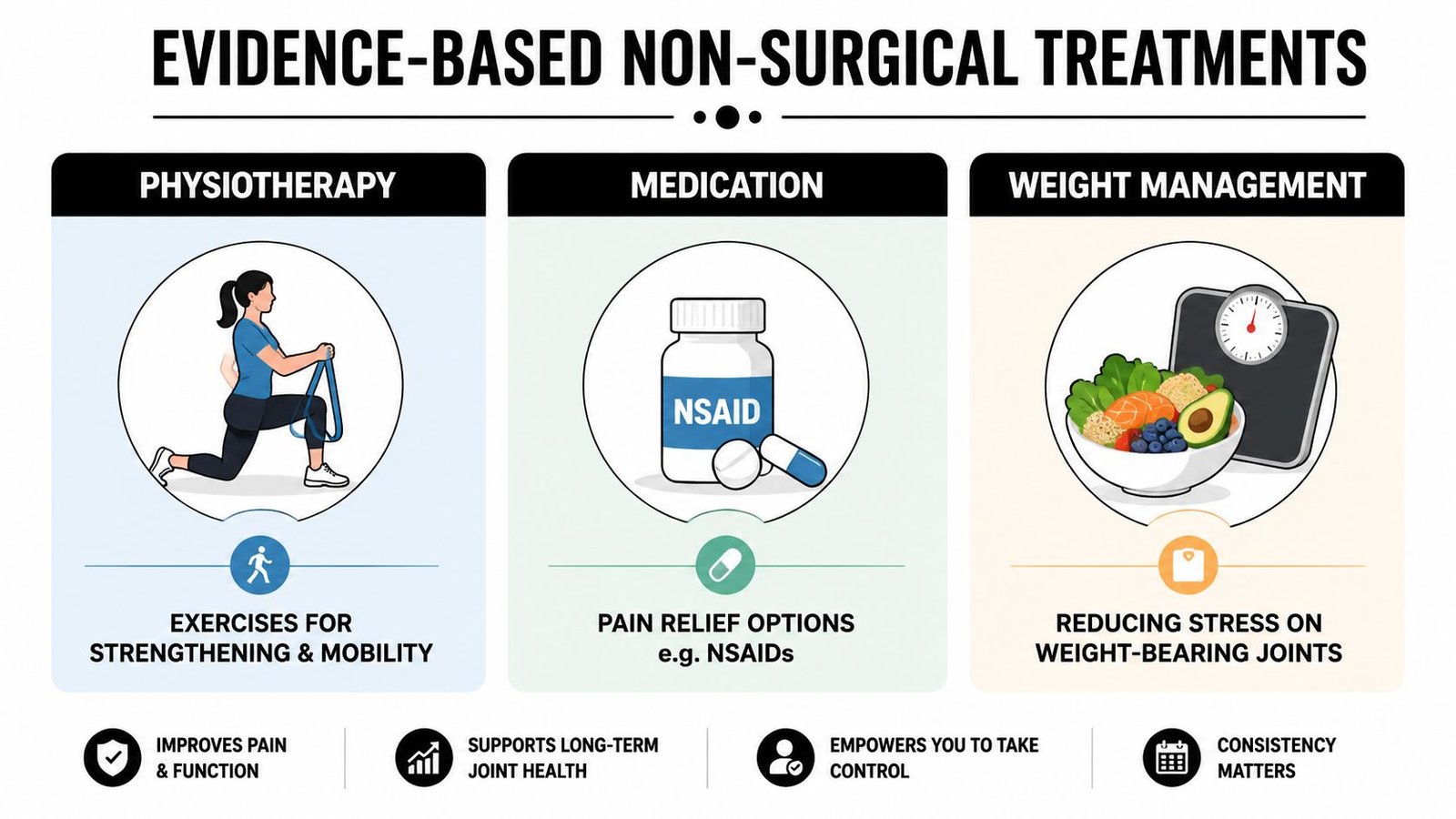
This is the in-between stage where good decisions matter. The aim is not to collect treatments. The aim is to choose the combination that improves walking, sleep, confidence, and day-to-day capacity.
A short explanation can help before comparing them in more detail.
How the main options compare
| Treatment | What It Involves | Primary Goal | Typical UK Availability |
|---|---|---|---|
| Osteopathy | Hands-on treatment, joint and soft tissue work, movement assessment, exercise advice | Reduce stiffness, improve movement quality, support function | Mainly private, some insurance pathways |
| Medical acupuncture | Needle-based pain management used alongside rehab and manual care | Help pain modulation and reduce protective muscle tension | Often private, sometimes within pain or physio services |
| Medication review | GP or specialist review of topical or oral medicines | Improve symptom control to support movement | NHS and private |
| Weight management support | Advice on reducing strain through sustainable lifestyle change | Lower joint stress and improve overall mobility | NHS and private |
What tends to work best in practice
Osteopathy can help when pain is being amplified by stiffness around the joint, altered gait, reduced spinal or pelvic movement, or protective muscle tension. I often see patients whose exercise plan is reasonable on paper but hard to carry out because the area is too guarded and uncomfortable. Hands-on treatment does not reverse arthritic change, but it can reduce resistance to movement and make rehabilitation more tolerable. In that role, it is a practical tool rather than a cure. For some patients, these knee osteoarthritis self-care and support strategies become far easier to follow once pain and stiffness have settled enough to let the knee bend, walk, and load more normally.
Medical acupuncture has a narrower role. It can be useful for short-term pain relief, especially when pain is disturbing sleep or keeping muscle tension high, but it works best as part of a wider plan. On its own, it rarely changes long-term function.
Medication review is often underused. If pain relief is either inadequate or causing side effects, the plan can stall. A GP, pharmacist, or specialist may be able to adjust timing, type, or dose so that movement work becomes more manageable.
Weight management support is relevant when load through the joint is part of the problem, but this needs careful handling. Telling someone to lose weight without helping them move more comfortably is not much use. Pain often has to settle enough first for activity to become realistic.
The best treatment is the one that matches the current barrier. Weakness needs progressive strengthening. Stiff, guarded movement may need pain relief or hands-on treatment first. Often both are true.
One private example of this type of service is Laurens Holve Healthcare, which provides osteopathy and acupuncture for musculoskeletal pain, including osteoarthritis-related symptoms. For patients in the gap between basic self-care and specialist intervention, that kind of setup can be useful because assessment, manual treatment, and exercise advice sit in one place.
The strongest non-surgical plans usually combine methods rather than relying on one. Exercise builds long-term capacity. Manual treatment may improve access to movement. Medication can make the process bearable enough to stick with. The trade-off is time, cost, and consistency. NHS care often gives good clinical oversight but may involve waits or shorter appointments. Private care may offer faster access and more hands-on time, but you need a clear reason for paying for it.
Navigating NHS vs Private Osteoarthritis Care
You speak to your GP, start basic self-care, and try to keep going. A few weeks or months later, the joint still hurts, walking is limited, and you are stuck in the part of the process that confuses many people. You are not ready for surgery, but self-management alone is not getting you far enough.
That is usually the key decision point. The question is less “NHS or private?” and more “What help do I need next, and how quickly do I need it?”
What the NHS pathway usually looks like
On the NHS, osteoarthritis care usually starts with a GP or, in some areas, a first contact physiotherapist. The first job is to check the diagnosis, screen for anything that does not fit a straightforward osteoarthritis pattern, and rule out causes of joint pain that need a different response. After that, the usual route is conservative treatment first, with advice, pain relief, physiotherapy, and review over time.
That sequence is sensible. It protects patients from being pushed too quickly toward scans, injections, or surgery when simpler treatment may still help.
The trade-off is access. Appointment length, waiting times, and referral pathways vary by area. A treatment can be appropriate and still take time to arrange. Some services are available in one region and hard to get in another. For patients whose pain is disrupting sleep, work, or confidence with movement, that delay can matter.
Common strengths of the NHS route include:
- Medical oversight: useful when diagnosis is uncertain, medication needs adjusting, or other health conditions affect treatment choices
- Joined-up escalation: if symptoms worsen, there is a clearer route back to the GP, community physio, or onward referral
- Lower financial pressure: you can work through options without paying at each step
What private care changes
Private care usually changes access, time, and continuity.
You can often get an appointment sooner. Sessions are often longer. The same practitioner may follow the case from the first assessment through the next stage of exercise progression, flare-up management, and decisions about whether further medical input is needed.
For someone in the gap between basic advice and surgical referral, that can be useful. Osteoarthritis treatment often works best when the plan is adjusted as the joint settles, rather than delivered as a fixed set of generic exercises and then stopped. A private osteopath, physiotherapist, or musculoskeletal clinician may have more room to do that.
Private care also has limits. It costs money, quality varies, and faster access is only worth paying for if the assessment is sound and the plan is realistic. Hands-on treatment can help some patients move more easily, but it should support function, not replace strengthening, pacing, or medical review where needed. If you want a practical example of how private care may fit into a knee osteoarthritis plan, this guide on treatment options for knee arthritis sets out where hands-on care and exercise advice can sit.
How to choose carefully
Choose based on clinical reasoning, not marketing.
Ask what the practitioner thinks is driving your pain now. Ask what they expect to improve first. It may be walking tolerance, stair confidence, morning stiffness, or the ability to restart exercise. Good answers are specific.
Check the basics:
- Professional registration: osteopaths should be registered with the General Osteopathic Council
- Assessment quality: they should ask about function, aggravating factors, irritability, goals, and general health, not just the painful joint
- Plan beyond the first session: a clear explanation of what happens if you improve, plateau, or flare up
- Willingness to refer: good private clinicians know when a patient needs GP review, imaging, injection discussion, or orthopaedic input
“If this treatment is the right fit, what should change over the next two to six weeks?”
A good answer gives you a way to judge progress. That matters more than promises.
When to Consider Injections and Joint Surgery
Injections and surgery sit later in the pathway. They’re not failures. They’re just different levels of intervention, and they make most sense when the simpler layers of treatment haven’t delivered enough relief.
Where injections fit
For some people, an injection is considered when pain remains high despite exercise, pacing, and appropriate practitioner-led care. The aim is usually to reduce pain enough to restore function, not to provide a permanent fix.
In the UK, people often ask about corticosteroid injections and hyaluronic acid. The practical point is that availability and recommendation are not the same for every option. Public-facing UK information is often patchy, and NHS access varies. Bupa notes that hyaluronic acid has mixed evidence and is not recommended on the NHS, while Arthritis UK notes that arthroscopic lavage is normally only available privately in the UK within its overview of evolving procedures for early osteoarthritis. That same page also notes that Autologous Chondrocyte Implantation is now available on the NHS for selected patients with small areas of cartilage damage or early osteoarthritis.
That tells you something important. Injection and procedure decisions are highly stage-dependent. What fits one patient may be inappropriate for another.
When surgery becomes a reasonable discussion
UK osteoarthritis care has shifted away from routine surgery as an early answer. A major policy review of osteoarthritis care in the UK reported that NICE tightened guidance on arthroscopic surgery, restricting it to people with mechanical symptoms such as locking or giving way, and this change aimed to reduce low-value procedures in favour of more appropriate management in its economic and policy review of UK osteoarthritis care.
If you’re reading about knee arthritis symptoms and treatment choices, that’s the key context to keep in mind. Surgery is usually discussed when pain is persistently limiting quality of life, function is clearly reduced, and well-run conservative care hasn’t been enough.
Typical reasons to seek an orthopaedic discussion include:
- Walking distance keeps shrinking
- Sleep is regularly disturbed by joint pain
- You can’t manage stairs, work, or daily tasks reliably
- You’ve tried appropriate conservative treatment without enough improvement
Surgery can be life-changing for the right patient. It is not the starting point for most.
Your Osteoarthritis Questions Answered
Can osteoarthritis be cured
A common pattern is this. The pain starts to affect walking, sleep, or stairs, and the next question is whether there is a treatment that can get rid of osteoarthritis completely.
At present, treatment is aimed at control rather than cure. The practical goal is to settle pain, improve joint capacity, and keep you doing the things that matter for as long as possible. In clinic, the people who do best are usually the ones who stop searching for a single fix and start building a plan they can follow.
That plan often includes load management, targeted exercise, weight loss where relevant, and review if symptoms change.
Do supplements help
Supplements are a frequent question, especially glucosamine and chondroitin. As noted earlier, they are not routinely recommended in standard UK osteoarthritis care because the evidence for meaningful benefit is weak.
Some people still choose to try them privately. That is a personal choice, but it is sensible to set a limit on cost and time. If you try a supplement, be clear about what you want it to change, such as pain on stairs or morning stiffness, and stop if there is no obvious benefit.
In practice, money is often better spent on good assessment, exercise support, footwear advice, or weight-management help.
What is the best exercise
The best exercise is the one your joint can tolerate consistently and progress from.
For one person, that may be sit-to-stands from a higher chair. For another, it may be cycling because walking is still too aggravating. For someone with a very irritable joint, pool-based exercise or short bouts of slower walking may be the right starting point. The detail matters because osteoarthritis management works best when the exercise matches the joint, the stage, and the current flare pattern.
If an exercise predictably stirs things up for days, it is the wrong starting dose, even if the exercise itself is reasonable.
Should I rest when it flares
Usually, symptoms settle better with modification than with complete rest. Reduce the load for a few days, keep some gentle movement going, and use simple measures such as heat if they help.
Complete rest often leaves the joint stiffer and confidence lower.
A flare should still behave like a flare. If pain becomes sharply different, swelling is unusual, the joint gives way more often, or you cannot put weight through it as normal, get reassessed rather than assuming it is only arthritis.
How do I know when self-care is no longer enough
This is the point many people get stuck on. They are not ready for surgery, but basic advice from a leaflet or a short GP appointment has not solved the problem either.
That in-between stage usually needs more specific input. Signs include repeated flares, shrinking walking distance, avoiding activities you used to manage, uncertainty about which exercises are helping or aggravating things, and relying more on pain relief without making real progress. At that stage, the next step is usually not to jump straight to injections or surgery. It is to get a clearer diagnosis, a practical plan, and a realistic sense of which treatment route fits your situation.
If you’re stuck in that in-between stage where basic self-care hasn’t been enough but you want to avoid unnecessary medication, injections, or surgery, Laurens Holve Healthcare offers Osteopathy and acupuncture in North London and Woking for people with osteoarthritis and other persistent joint problems. A thorough assessment can help clarify what’s driving your pain and whether a hands-on, exercise-supported plan is the right next step.




