You’ve been told it isn’t plantar fasciitis, but the pain is still there. It catches you when you walk to the kitchen, nags through a commute, or flares after a long day standing. By this point, many individuals aren’t looking for another generic list of foot conditions. They want to know what the pain might be, what signs matter, and what to do next.
That’s a sensible instinct. Pain in arch of foot not plantar fasciitis is a real clinical problem, not a technicality. The arch is a hard-working, load-bearing part of the foot, and several different tissues can produce very similar symptoms. The key is to stop chasing the wrong label and start narrowing down the pattern.
Table of Contents
- Is It Really Plantar Fasciitis?
- How to Tell Your Arch Pain is Not Plantar Fasciitis
- Five Common Causes of Arch Pain (That Aren’t Plantar Fasciitis)
- Simple Self-Assessments and Critical Red Flags
- Effective Conservative Treatments You Can Start Today
- Finding a Lasting Solution With Professional Help
Is It Really Plantar Fasciitis?
A common story goes like this. Someone develops pain under the foot, searches online, sees plantar fasciitis everywhere, buys an insole, stretches the calf, and waits. But the pain doesn’t behave the way plantar fasciitis usually does. It isn’t mainly at the heel. It spreads through the middle of the arch. It gets worse as the day goes on. Sometimes it burns, tingles, or feels oddly deep.
That mismatch matters.
Classic plantar fasciitis usually centres more around the heel and often has a very recognisable pattern. The first few steps after rest are commonly the worst. When pain sits further forward in the arch, or when the symptoms feel broad, hot, burning, or nerve-like, clinicians need to think wider. If you want a clearer picture of the usual heel-pain pattern, this guide on understanding and treating plantar fasciitis is useful for comparison.
According to Foot Health Facts on arch pain, the arch is a load-bearing structure, and when symptoms are centred away from the heel, clinicians are pushed toward alternative diagnoses instead of assuming plantar fasciitis. That matters in practice because midfoot arthritis, tendon overload, stress injury, and nerve entrapment can all mimic “arch pain”.
Many patients are right when they say, “This doesn’t feel like the heel pain I’ve read about.”
In clinic, the important question isn’t “What’s the name of the pain?” It’s “Which structure is being overloaded, irritated, or failing to support the foot properly?” Once you ask it that way, the next steps become much clearer.
How to Tell Your Arch Pain is Not Plantar Fasciitis
You get out of bed, take a few steps, and the arch feels noticeable but not terrible. By late afternoon, after commuting, standing at work, or walking the dog, it is far more irritated. That pattern should make you pause before accepting plantar fasciitis as the full answer.
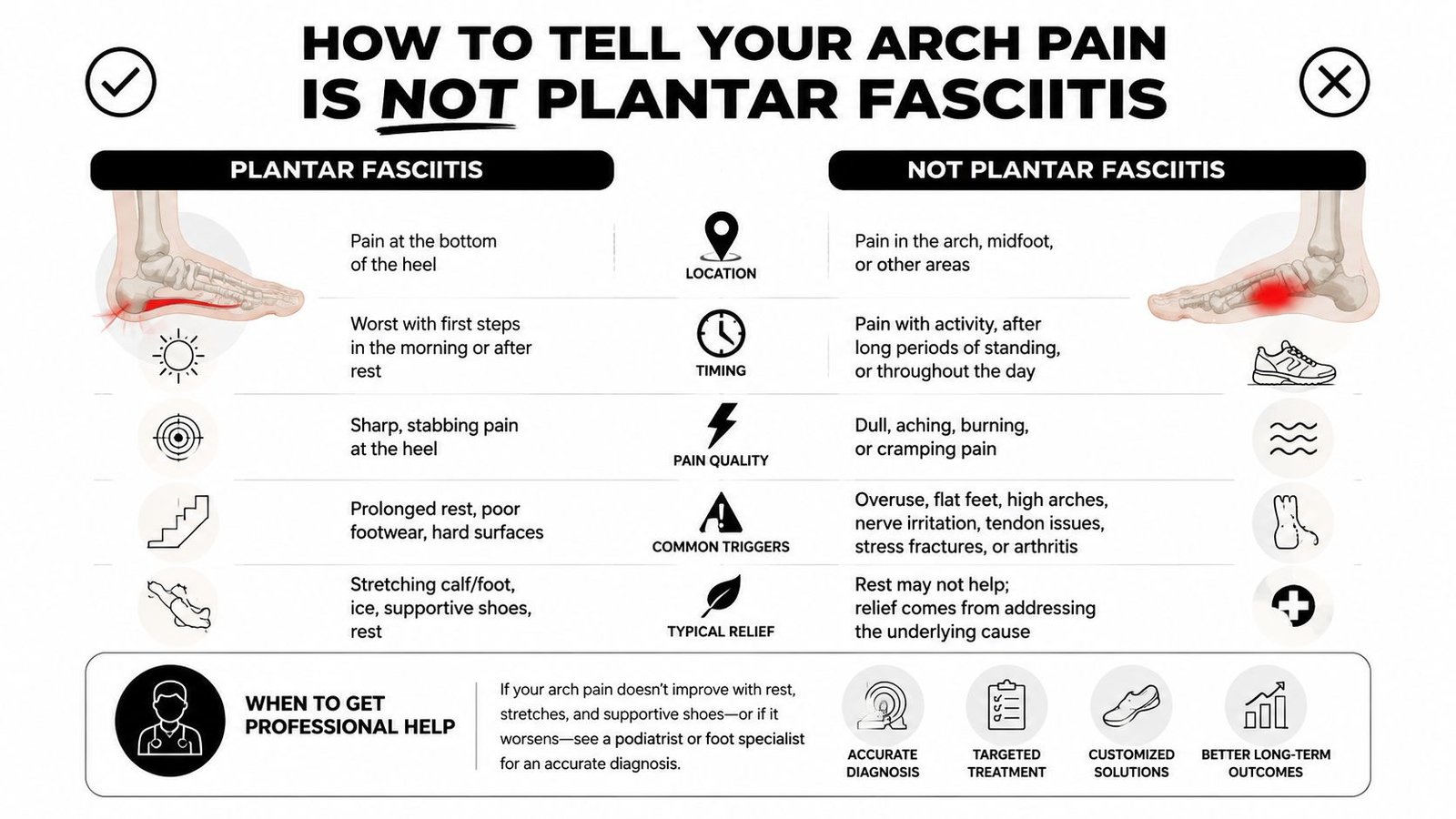
A practical way to sort arch pain is to check three things. Where it sits. When it flares. What it feels like. In clinic, those three clues often tell you whether the plantar fascia is really the main problem or whether a tendon, joint, nerve, or bone needs more attention.
Look at where the pain sits
Plantar fasciitis usually stays closest to the inner heel, even if it spreads a little into the arch. Pain that sits further forward in the middle of the arch, tracks behind the inner ankle, or spreads across the midfoot deserves a wider view.
Pain behind the inner ankle and down the inside of the arch often fits a tendon problem more than fascia irritation. A deep, stiff ache in the centre of the foot can fit irritated joints. A very localised sore spot over one bone needs more caution, especially if walking or hopping makes it sharply worse.
If the discomfort is drifting towards the ball of the foot rather than the heel, it may help to compare it with other patterns of metatarsalgia or forefoot pain, because patients often describe that area loosely as “the arch”.
Notice when it hurts most
Timing matters.
Classic plantar fasciitis often has a clear morning pattern. The first few steps after rest are usually the sharpest, then it eases as the tissue warms up. Arch pain from tendons, joints, or stress irritation often behaves differently. It may be tolerable early on, then build with standing, longer walks, hills, hard floors, or cumulative load through the day.
That distinction is not perfect, but it is useful. If your pain is mainly a later-in-the-day problem, or it ramps up with activity rather than easing into it, I would be slower to label it plantar fasciitis without looking further.
Pay attention to the type of pain
The quality of pain gives another clue.
| Symptom | Classic Plantar Fasciitis | Likely Another Cause |
|---|---|---|
| Main site | Inner heel, sometimes extending into nearby arch | Mid-arch, behind inner ankle, across midfoot, or a focal bony point |
| Typical timing | First steps after rest are often worst | Worse with prolonged standing, walking, later in the day, or with training load |
| Pain quality | Sharp, stabbing, tight | Aching, burning, tingling, deep dull pain, or pinpoint tenderness |
| Visible change | Usually little change in foot shape | Flattening arch, swelling, altered foot posture, or limp |
| What it suggests | Plantar fascia irritation | Tendon problem, nerve irritation, joint problem, or stress injury |
A burning or tingling sensation raises the possibility of nerve irritation. A heavy, tired ache along the inside of the arch points more towards a support structure, often a tendon. A deep pain that feels “inside the foot” can fit the joints of the midfoot. Pinpoint tenderness over one spot is the pattern I treat more carefully, because stress injuries are easy to miss if the foot is called “inflamed”.
A few quick checks help:
- Pain mainly at the inner heel first thing keeps plantar fasciitis in the picture.
- Pain that builds with use points more towards tendon or joint overload.
- Burning, tingling, or altered sensation makes nerve involvement more likely.
- Swelling, flattening of the arch, or a limp means the problem needs a more careful assessment.
- A single bony tender point should be treated as a possible stress injury until assessed.
Practical rule: if the pain is centred away from the heel, behaves badly later in the day, or feels burning, deep, or pinpoint rather than tight and heel-based, stop assuming every arch pain problem is plantar fasciitis and get the diagnosis checked properly.
Five Common Causes of Arch Pain (That Aren’t Plantar Fasciitis)
Some diagnoses overlap, and more than one problem can exist at the same time. Still, these five patterns come up again and again.
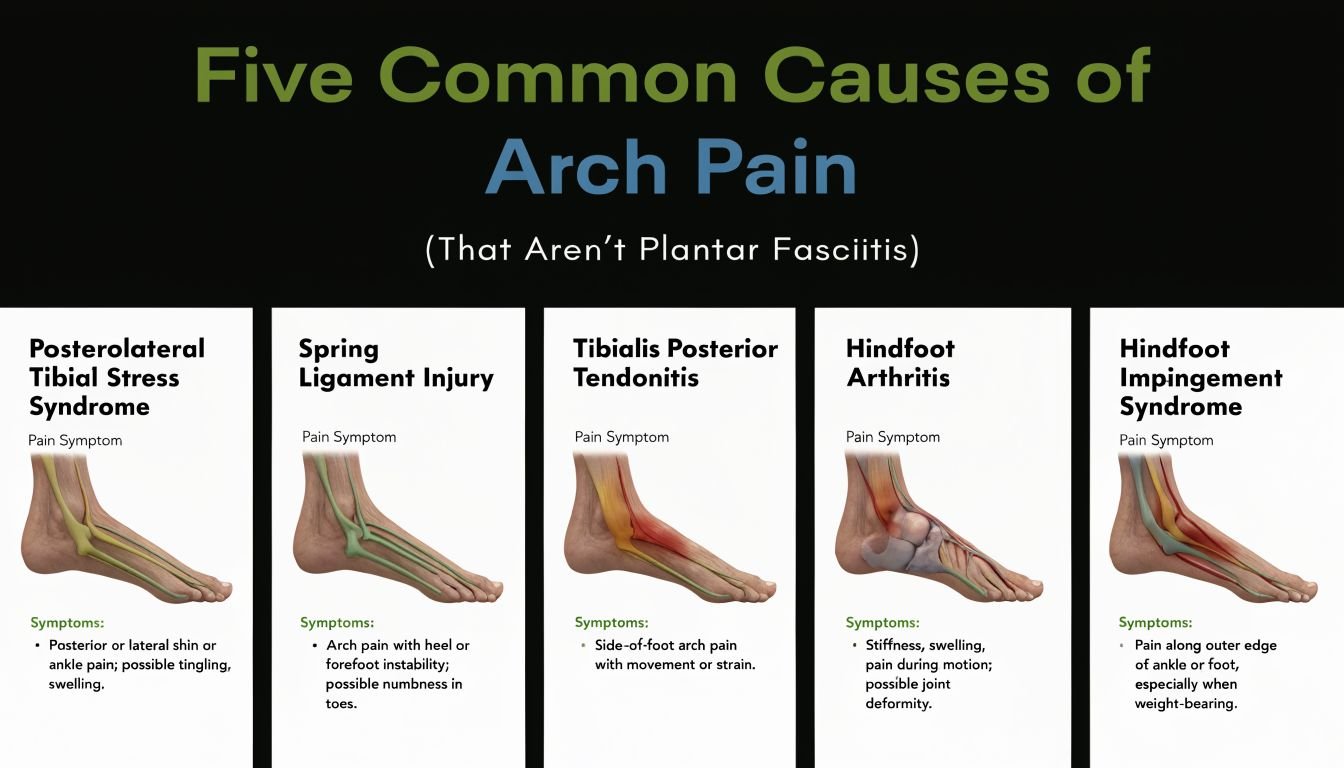
Posterior tibial tendon dysfunction
This is one of the most important alternatives to plantar fasciitis. The posterior tibial tendon helps support the inner arch. When it becomes overstretched, inflamed, or partly torn, the foot can start to overpronate and the arch may gradually flatten.
The pain usually sits along the medial arch and may also run behind the inner ankle bone. People often describe an aching or burning discomfort rather than a sharp heel stab. Walking longer distances, climbing stairs, or standing for long periods commonly aggravates it.
A UK audit summarised in foot arch pain guidance found that 18% of referrals with medial arch pain and flexible flatfoot met criteria for early-stage PTTD, and females over 40 and individuals with a BMI above 27 had 3 to 4 times higher odds. That’s a useful reminder that not every “fallen arch” is harmless.
What makes it different:
- The arch may look lower
- Heel alignment may drift outward
- Single-leg heel raise is often weak or painful
If there’s also pain towards the front of the foot, this guide on metatarsalgia or forefoot pain can help separate arch symptoms from ball-of-foot pain.
Flexor tendon irritation
This tends to be less dramatic than PTTD but still very limiting. The flexor tendons run under and around the foot, helping control the toes and support the arch during push-off.
The pain often feels like a pulling or aching strain in the arch, especially during walking, running, or after a sudden jump in activity. It may follow a change in footwear, hill walking, return to sport, or long periods on hard floors.
This pattern is more likely when:
- The pain is activity-related
- The foot feels tired rather than unstable
- You don’t have much burning, numbness, or major shape change
In practical terms, people often make this worse by stretching aggressively into pain or by massaging the sore area too hard. Tendons usually respond better to load reduction first, then controlled strengthening later.
Tarsal tunnel syndrome
This is a nerve entrapment problem on the inside of the ankle and foot. It can produce arch pain, but the feel is different. Instead of a simple mechanical ache, people often report burning, tingling, buzzing, shooting pain, or numbness into the sole.
Symptoms may worsen with standing or walking for longer periods. Some people notice it more by evening. Because the nerve can refer symptoms into the arch, it’s easy to mistake it for a fascia problem.
Clues that push this higher on the list:
- Pins and needles in the sole
- Sensitivity around the inside of the ankle
- Pain that feels electrical rather than tight
When pain comes with tingling or numbness, think nerve until proven otherwise.
Tarsal tunnel syndrome also needs a bit more caution because treating it as a simple overload problem can delay useful assessment.
Midfoot arthritis
This is a common reason for stubborn, central arch pain in adults, especially when the symptoms have been around for a long time. The joints involved are often the tarsometatarsal or nearby midfoot joints.
The pain is usually a deep, dull ache centred in the midfoot and medial arch. Hard surfaces, longer walks, and weight-bearing tend to make it worse. Some people notice swelling or stiffness through the front and middle of the foot.
A UK multicentre registry report on chronic midfoot pain found that 32% of adults aged 45 to 75 presenting with chronic midfoot pain had radiographically confirmed midfoot arthritis, with a mean symptom duration of 18 months before specialist referral. That delay is common. Many people assume they just have a “tight arch” and keep trying short-term fixes.
This diagnosis becomes more likely if:
- You’re over 50
- The foot feels stiff as well as sore
- Walking on hard ground is especially aggravating
- There’s a history of midfoot sprain, flatfoot, or long-standing overload
Metatarsal stress fracture
Stress injuries don’t always sit exactly where people expect. A metatarsal stress fracture can refer discomfort into the arch or present as pain under the middle or front part of the foot that people loosely call “arch pain”.
This tends to show up after a load spike. More walking than usual, a return to running, a holiday with long daily mileage, or an abrupt training change are classic stories. The pain often starts as something mild and then becomes more localised and sharper.
Typical pointers include:
- A very specific tender point
- Pain with impact or push-off
- Symptoms that settle with rest but return quickly with activity
This is one of the reasons I’m cautious when someone says their “plantar fasciitis” came on after a sudden training jump and is now easy to locate with one fingertip. Bone stress needs different management from tendon overload.
Simple Self-Assessments and Critical Red Flags
You can do a few basic checks at home. They won’t diagnose you, but they can help you decide whether this looks like a simple overload problem or something that deserves quicker assessment.
Self-checks you can do safely at home
Start with a mirror and a short walk barefoot across the room.
- Compare both arches: Does one look flatter, lower, or more collapsed than the other?
- Check the inside ankle area: Is there soreness behind the inner ankle bone as well as in the arch?
- Do a single-leg heel raise: Hold onto a wall and try rising onto the ball of one foot. If it’s clearly weak, painful, or your heel drifts outward, posterior tibial tendon trouble moves up the list.
- Palpate gently: A broad tender area suggests soft tissue overload. One exact bony point deserves more caution.
- Notice nerve symptoms: Burning, tingling, or numbness should make you consider whether a pinched nerve or nerve irritation pattern is involved rather than a simple fascia strain.
None of these tests should be forced. If a movement sharply increases pain, stop.
Red flags that need prompt assessment
Some symptoms move this out of the self-care category.
According to UK guidance discussed in this foot pain triage article, NICE treats unexplained bone pain, night pain, or persistent symptoms as red flags needing prompt medical assessment, while NHS guidance advises urgent review for severe pain, swelling, deformity, or inability to bear weight.
Seek prompt medical advice if you have:
- Severe pain or rapid swelling
- Visible deformity
- Inability to bear weight
- Pain that wakes you at night
- Numbness that’s worsening
- Persistent unexplained bone pain
Don’t keep self-treating a foot that’s becoming harder to walk on.
In the UK, that may mean urgent care for acute severe symptoms, or your GP for assessment and onward referral if the problem is persistent, unclear, or suspicious for stress injury, inflammatory disease, or significant tendon damage.
Effective Conservative Treatments You Can Start Today
You get the most benefit from early treatment when it matches what the foot is reacting to. Until you have that clearer, the safest approach is to reduce strain, support the arch better, and avoid the common mistake of throwing generic plantar fasciitis advice at every kind of arch pain.
Reduce the load that is keeping it irritated
The first job is simple. Stop repeating the activity that keeps stirring it up.
That may mean shorter walks for a week, fewer runs, breaking up long standing periods at work, or using lifts instead of stairs for a few days if push-off is painful. Relative rest works better than trying to completely immobilise yourself, but it does need to be real. If every day still includes the same painful walk, the foot usually stays stuck in the same cycle.
A practical rule is this: keep activity within a level that settles reasonably quickly afterwards. If your pain builds through the day and is worse again the next morning, the load is still too high.
Choose support that controls movement
For arch pain, softness is often overrated. Slippers, unsupportive trainers, and worn-out shoes can feel comfortable briefly but let the foot collapse or twist more than the irritated tissue can tolerate.
Start with:
- A supportive lace-up shoe with a stable sole
- Avoiding barefoot time on hard floors
- A simple off-the-shelf arch support if it feels clearly better in it
- Temporary taping if it reduces pain while walking
Flat feet, high arches, and stiff midfoot mechanics can all change how force travels through the arch. The practical point is not to chase a perfect foot type. It is to find footwear that makes walking easier and symptoms calmer.
If symptoms have been going on for a while, or there is concern about whether the problem is tendon, joint, or bone, imaging is sometimes part of the next step. This guide on whether an MRI or X-ray is best for foot pain explains when each is more useful.
Use symptom relief with some restraint
Ice can help after activity if the foot feels hot, puffy, or reactive. Elevation can help if there is mild swelling around the area. These are comfort measures. They do not solve the reason the arch is being overloaded.
Gentle calf mobility can be useful if the ankle feels stiff and walking is forcing extra strain through the arch. Stretching should not reproduce sharp pain, tingling, or a strong pulling sensation directly through the sore spot. If it does, stop. That pattern often points away from a simple tight-calf problem.
What commonly slows recovery:
- Deep massage into a tender arch
- Repeated stretching because “it must be plantar fasciitis”
- Trying to strengthen through pain too early
- Switching to minimalist shoes while the foot is still irritated
Add strength only when the foot is settling
Once day-to-day pain has eased, simple strengthening can help the foot tolerate load again. This matters most when the problem is linked to tendon overload or poor control through the ankle and arch.
Useful starting points include:
- Slow calf raises, if they do not provoke arch pain
- Toe control exercises
- Single-leg balance near a wall or kitchen counter
- Gradual return to walking volume rather than jumping back to full distance
I usually advise patients to judge progress by function, not just pain in the moment. If walking becomes easier, morning soreness is less severe, and the foot settles faster after activity, the plan is probably heading in the right direction.
Better shoes, lower load, and sensible rehab can settle many cases. Persistent pain still needs a proper diagnosis.
Finding a Lasting Solution With Professional Help
Once you’ve ruled out the obvious red flags, the next decision is who should assess it. For persistent pain in arch of foot not plantar fasciitis, the right clinician should look at more than the painful spot. They need to assess how the foot is loading, whether the arch is being supported well enough, and whether the problem is tendon, joint, nerve, or bone.
Why diagnosis changes treatment
A strained tendon needs a different plan from arthritic midfoot joints. A nerve problem needs a different plan from a stress fracture. That sounds obvious, but many people still spend weeks doing the same stretches and using the same internet advice for completely different conditions.
As noted in this discussion of biomechanical overload and arch pain, both flat feet and high arches can overload the foot, and practical management often comes back to structured rehab, weight management, and shoe changes rather than simple remedies. That’s why a proper biomechanical assessment is worth it.
An osteopathic assessment should usually include:
- Walking and standing mechanics
- Arch height and heel alignment
- Calf, ankle, and foot strength
- Mobility through the midfoot and ankle
- Whether imaging might be needed
If imaging is being discussed, this overview of MRI vs X-ray and what each is best for helps explain why the choice depends on the suspected tissue.
Who to see in the UK and when
A GP is the right first stop when red flags are present, when pain is persistent and unexplained, or when imaging and medical referral may be needed. A podiatrist is often useful when footwear, orthoses, pressure distribution, or foot-specific mechanics are central. An osteopath can be helpful when the problem is mechanical, load-related, and tied to the way the foot, ankle, calf, knee, and hip are working together.
One option for people in Highgate or Woking is Laurens Holve Healthcare, where assessment and treatment for foot and ankle pain can include hands-on care, exercise guidance, and referral onward when scans or consultant input are needed.
The point isn’t to collect opinions from three different places. It’s to get a clinician who can say, with reasonable confidence, “This looks like tendon overload,” or “This needs imaging,” or “This isn’t behaving mechanically and should be medically reviewed.”
If your arch pain has already been labelled “not plantar fasciitis” but you still don’t know what it is, the next step is a proper assessment rather than more guesswork. Laurens Holve Healthcare sees patients in North London and Woking, Surrey for osteopathy and acupuncture, including foot and ankle problems where biomechanics, tendon overload, joint stiffness, or nerve irritation may be involved.




